

Here is a small, useful test. Ask any peptide provider one question: who decides my dose, and how. If the answer is a price list, you already have your answer about the provider. This piece is built around that question, broken into five checkable signals, because the price tag is the one number that tells you almost nothing about whether the dosing behind it makes sense.
The habit worth breaking is shopping by monthly cost first. Cost is an output. It is downstream of decisions about prescribing, monitoring, and quality control that mostly happen out of view. Score those decisions instead, on a simple 0-to-2 scale across five signals, for a possible ten points. A provider that cannot clear the midpoint isn’t a bargain. It’s the absence of the very things that make a dose meaningful, with a lower number attached.
The claim under all of this: dose is not a fact, it’s a curve
Start with what the trial data actually show, because it reframes the whole exercise.


The claim: peptide dosing is precise and the number on the syringe is what matters.
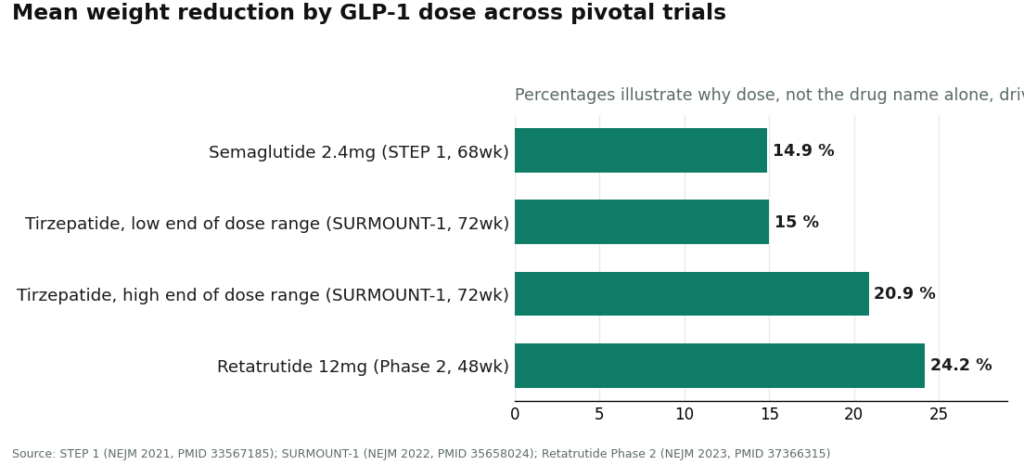
The evidence tier: studied, and studied specifically as a range, not a point. In the SURMOUNT-1 trial, tirzepatide produced mean weight reductions from 15.0% to 20.9% across its dose range over 72 weeks, against 3.1% on placebo [2]. In STEP 1, semaglutide at 2.4 mg weekly produced a 14.9% mean reduction at 68 weeks against 2.4% on placebo [1], and that 2.4 mg endpoint was reached by titrating up over weeks, not by starting there. The investigational triple agonist retatrutide hit a 24.2% mean reduction at its 12 mg dose at 48 weeks in a phase 2 trial [3].
The honest bottom line: these numbers are dose-response curves, not fixed facts. Five to six points of separation between the low and high tirzepatide doses is not noise, it’s the mechanism. Whoever controls where you sit on that curve controls a meaningful share of your outcome and your side-effect risk. That is not a detail buried in an appendix. It is the reason the next five signals exist.
Signal 1: Is a licensed clinician actually setting the dose?
The claim: a prescription means someone is managing your dose.
The evidence tier: wildly variable in practice. Score a 2 if a licensed clinician evaluates you personally, sets a starting dose, and has an articulated plan for titrating it up or down. Score a 1 if a clinician exists somewhere in the process but the dosing is a fixed template applied to everyone. Score a 0 if there’s no clinician at all, just a label suggesting a “research” amount.
The honest bottom line: the trials above worked because clinicians managed titration deliberately. A provider replicating that structure is offering something close to the studied version of the therapy. A chatbot questionnaire is not a prescriber, no matter how it’s marketed, and a provider that lets you believe otherwise has already failed the honesty test that shows up later in this list.
Signal 2: Does the dose adjust to you, or does everyone get the same ladder?
The claim: dosing is personalized.
The evidence tier: ask, don’t assume. Score a 2 if your dose reflects your starting point and your actual response, with room to slow down if you’re struggling. Score a 1 if adjustment exists but is basically a standard step-up schedule applied uniformly. Score a 0 if the schedule is identical for every patient regardless of how anyone is doing.
The honest bottom line: side effects in this drug class tend to be dose-paced, meaning tolerability often comes down to speed of titration, not just final dose. A flat protocol assumes every body responds identically, which none of the cited trials assumed. The tell is a single question: what happens if this dose is too much for me, and who makes that call. A provider with a real answer scores well. One that points back at a label does not.
Signal 3: Does anyone check back in?
The claim: dosing is a decision made once, at intake.
The evidence tier: this is arguably the weakest link industry-wide. Score a 2 if there’s scheduled follow-up, a channel to report how you’re responding, and an actual mechanism to adjust or stop. Score a 1 if follow-up technically exists but only if you go chase it yourself. Score a 0 if the relationship ends the moment the package ships.
The honest bottom line: the correct dose is rarely obvious on day one. It gets discovered by watching a response over weeks, which means the feedback loop is where the real dosing decisions happen, not the intake form. A structured way to log that response, rather than relying on vague memory, is what turns “I think this is working” into something a clinician can actually act on. FormBlends, as one example, pairs its supervised-access model with a tracker app for logging protocol data over time. That’s cited here as an illustration of what the signal looks like when it’s present, not a recommendation to buy anything. A provider with no follow-up mechanism cannot catch an overshot dose early, and it cannot capture room to safely go further either, because it has no visibility into you after checkout.
Signal 4: Can the product’s contents be verified?
The claim: the vial contains what the label says.
The evidence tier: this is where “precise” dosing quietly becomes fiction. Score a 2 if the medication comes from a licensed pharmacy running actual quality steps, purity and identity testing among them. Score a 1 if some quality documentation exists but it’s controlled entirely by the seller, not an independent party. Score a 0 if the only assurance is a certificate the vendor decided, unilaterally, to include.
The honest bottom line: a beautifully titrated plan executed on an unverified vial isn’t precision, it’s the appearance of precision. If the true concentration is uncertain, the number written on the syringe doesn’t correspond to anything reliable in your body. This signal is easy to skip past because it doesn’t feel like a “dosing” question. It is one, possibly the one that matters most once the other four are in order.
Signal 5: Does the provider tell you what’s actually known, versus what’s assumed?
The claim: everything in the catalog works and is safe.
The evidence tier: deliberately uneven across compounds, and that unevenness is the whole point of this signal. Score a 2 if a provider clearly separates the well-studied compounds from the barely-studied ones and says plainly when something is investigational or compounded rather than FDA-approved. Score a 1 if the framing is broadly honest but leans optimistic. Score a 0 if the entire catalog is presented as settled science.
The honest bottom line: dosing confidence should track the size of the evidence base, and it often doesn’t. A GLP-1 with large randomized trials behind it has a real basis for a target dose [1][2]. BPC-157 does not: a 2025 narrative review describes the human evidence as “exceedingly sparse” and recommends treating the compound as investigational [4]. A provider that doses BPC-157 with the same confidence it applies to semaglutide is borrowing certainty it hasn’t earned, and that borrowed confidence is a risk to the person injecting it. The FDA states plainly that compounded products are not FDA-approved and have not been evaluated for safety, effectiveness, or quality [5]. A provider that repeats that fact instead of burying it earns the 2.
Adding it up
Total the five signals. The read is blunt, deliberately so.
An 8 to 10 describes a provider that prescribes individually, follows up, verifies its product, and tells the truth about what’s known versus assumed. That’s the studied version of this category of treatment, and it’s usually worth what it costs, even when a cheaper option exists next to it.
A 4 to 7 is a real provider with a real gap somewhere, a clinician but no follow-up, or quality documentation but no individualization. Use the low score to find the specific hole and ask about it directly before paying anyone.
A 0 to 3 is a vial with a shipping label and a price. The savings aren’t a discount, they’re the dollar value of everything the scorecard didn’t find. Every missing point is a protection you’re not getting.
Notice that price never entered the scoring. It comes in last, as a tiebreaker among providers that already cleared the bar. A high score at a fair price is the outcome worth wanting. A low score at any price is the trap, wearing a bargain’s clothing.
The compressed version
Good dosing is a system, not a number: a clinician sets it, it’s adjusted to the person, follow-up corrects it, a licensed pharmacy makes the concentration real, and the provider says out loud how much is actually known. Score those five things before the price column even opens, and the decision gets made on what actually determines whether the treatment works and whether it’s safe, rather than on the one number that was never measuring that in the first place.
Questions people actually ask
Why bother scoring a provider instead of comparing monthly price directly? Because price measures what leaves your bank account, not whether the dosing behind it is safe or supervised. The five signals here, prescriber, individualization, follow-up, verifiable quality, and honesty about evidence, are precisely what gets stripped out to make a cheap offer cheap. A low score at any price is a trap, since the discount is built from removing exactly what the scorecard checks for.
What’s the lowest score I should accept? Aim for 8 to 10. A 4 to 7 is workable, a real provider with an identifiable gap, so use the score to find that gap and ask about it directly. A 0 to 3 is a vial shipped with a price attached, where the low cost is just the sum of the missing protections.
Which single signal carries the most weight? Signal 1, whether a licensed clinician sets your dose and owns the titration plan. The trials that produced the strong percentages used clinician-managed titration, so a provider running the same structure is offering the studied version of the therapy. A questionnaire answered by software is not a substitute for a prescriber.
How do I check whether dosing is truly individualized, versus a fixed ladder dressed up as personal? Ask one direct question: if this dose is too much for me, what happens, and who decides. A provider that individualizes gives a specific answer with room to slow down. One running a flat protocol will point you back at the label, treating every patient as interchangeable, which the trial data never assumed.
Why does product quality belong in a conversation about dosing? Because an unverified vial makes the whole idea of “precise dosing” meaningless. If nobody’s confirmed the true concentration or purity, the number on the syringe is disconnected from what’s actually entering your body. A perfectly titrated plan built on unverified material only looks careful.
Should every peptide be dosed with equal confidence? No, and a provider implying otherwise is telling you something about their honesty, not the compound. Semaglutide and tirzepatide have large randomized trials behind their dose targets [1][2]. BPC-157, per a 2025 narrative review, has human evidence described as “exceedingly sparse,” and the compound is considered investigational [4]. A provider that dials back its confidence where the evidence is thin, and says so out loud, is the one earning the top mark on the fifth signal.
Primary sources
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks, reached by titration. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight reduction 15.0% to 20.9% across the dose range vs 3.1% placebo over 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023. PMID 37366315. Mean weight reduction 24.2% at the 12 mg dose vs 2.1% placebo at 48 weeks.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177. Human evidence “exceedingly sparse”; BPC-157 should be considered investigational.
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
How much does peptide therapy typically cost?
Most people land somewhere between $150 and $600 a month, depending on which peptide, what dose, and who’s supervising it. Compounded injectables like sermorelin or BPC-157 tend to sit toward the lower end. Stacking multiple peptides, or dosing more frequently, pushes the number up. Lab monitoring and follow-up visits add to the running total, and it’s worth budgeting for those from the outset rather than treating them as a surprise later.
How much does BPC-157 therapy cost specifically?
Through a physician-supervised compounding pharmacy, BPC-157 generally runs $80 to $250 per vial, with the monthly total depending on the schedule your provider actually writes. If a price sits well below that range online, it’s usually research-grade material sold without a prescription, a different category legally and qualitatively, not just a discount. The price gap tracks oversight, testing, and accountability, not just markup.
Does insurance cover peptide therapy?
Basically none of it, at present. Most compounded peptides are prescribed off-label, and insurers routinely exclude off-label compounded drugs from reimbursement. Some people run costs through an HSA or FSA when a licensed provider has written the prescription, but check with your plan administrator before assuming that will work.
Is peptide therapy worth the cost?
That depends heavily on what you’re treating and how straight your provider is with you about the evidence. Some peptides, growth-hormone-stimulating protocols among them, have a decent body of clinical data behind them. Others are early-stage, with thin human data. A provider willing to walk you through both the realistic upside and the evidence gaps, the way the physician-supervised model at FormBlends does, tells you more about likely value than one leading with before-and-after photos.
Written by Kaya Yang, features writer. Reviewing the trials and labels directly. Last reviewed February 2026.
Not medical advice. Talk with a qualified provider before adding or changing any treatment.



